by Dr. Rosanoff | Aug 1, 2022 | Magnesium Education
This mineral could benefit a wide array of ailments
“Magnesium is a remarkable mineral that doesn’t get anywhere near the credit it deserves for preventing and treating disease,” says Mary Ann Block, DO, founder and medical director of the Block Center in Fort Worth, Texas.
Magnesium is a cofactor in 80% of the body’s metabolic activities, including fundamentals such as energy production, blood sugar regulation, maintenance of electrolyte balance, muscle function, nerve function, protein synthesis, and DNA and RNA synthesis, says Andrea Rosanoff, PhD, director of research and science information outreach at the Center for Magnesium Education and Research in Pahoa, Hawaii. Research suggests that low magnesium levels are linked to hypertension, cardiovascular disease, and Type 2 diabetes.
Hypertension
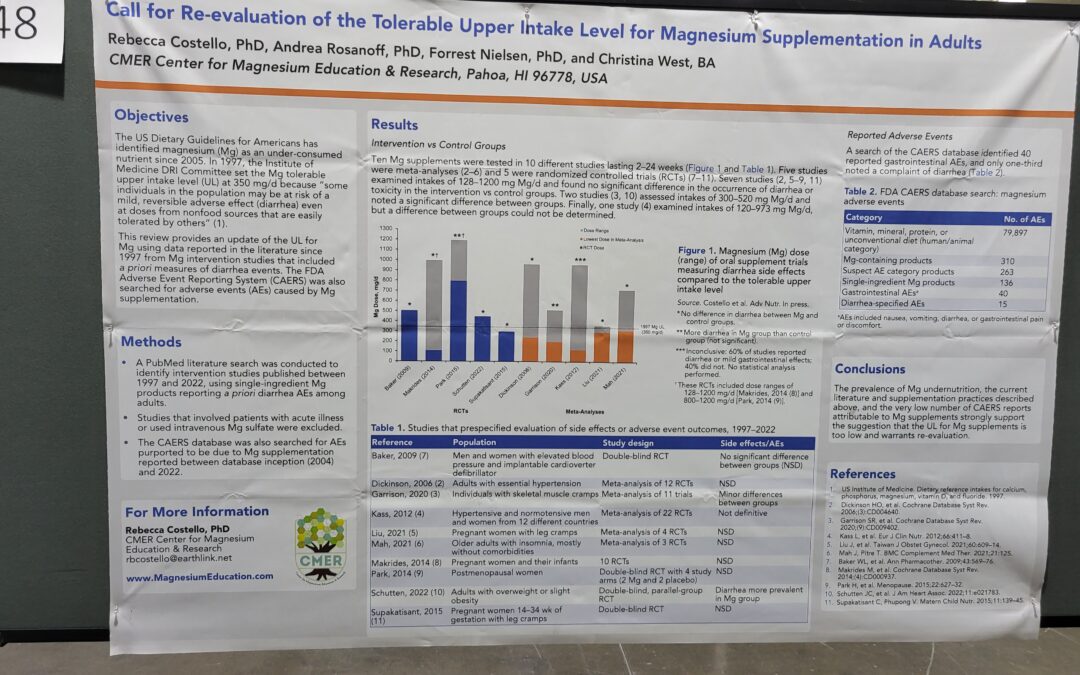
Nearly half of all American adults have high blood pressure, which is the No. 1 risk factor for heart attack and stroke. In a paper published in the American Journal of Clinical Nutrition, Dr. Rosanoff and her colleagues analyzed 11 studies on high blood pressure that, together, examined over 500 people with prediabetes, insulin resistance, or noncommunicable chronic diseases.
They found that people who took a magnesium supplement (365 to 450 mg daily) had a significant reduction in both systolic and diastolic blood pressure: a mean of 4.18 mm Hg systolic and 2.27 mm Hg diastolic.
Cardiovascular Disease
Magnesium can help prevent cardiovascular disease, says Dr. Rosanoff. In a study that she helped conduct, people at high risk for magnesium deficiency were also found to be at an increased risk for cardiovascular disease.2 Additionally, the study linked low levels of magnesium to systemic inflammation—a risk factor for cardiovascular disease and many other chronic diseases, according to a 2019 paper published in Nature Medicine.
Diabetes
Some research suggests higher magnesium intakes might be associated with improved blood sugar regulation. In an analysis published in the British Journal of Nutrition on January 20, 2022, researchers reviewed the results of 18 studies on magnesium and blood sugar levels. They determined that “oral [magnesium] supplementation could have an effect on glycaemic control in [Type 2 diabetes mellitus] patients,” but cautioned that “the clinical trials so far are not sufficient to make guidelines for clinical practice.”
In an analysis in the Journal of Human Nutrition and Dietetics, researchers found that magnesium supplementation had a favorable effect on cardiovascular risk factors associated with Type 2 diabetes, particularly among people with magnesium deficiency. They concluded: “Magnesium supplementation may decrease the risk [of Type 2 diabetes] associated cardiovascular diseases, although future large RCTs are needed for making robust guidelines for clinical practice.”
Other Health Problems
Perhaps due to the role magnesium plays in many systems and organs, some studies suggest that it might help with a range of other ailments, though the data is often inconclusive:
Insomnia. In a 2021 analysis of past studies, researchers determined that people who took magnesium supplements fell asleep faster and slept longer, though they cautioned that all of the trials they analyzed “were at moderate-to-high risk of bias and outcomes were supported by low to very low
quality of evidence.”
Migraines. A cross-sectional analysis published in Headache reviewed health data from more than 3,600 people and found that people who had higher magnesium intakes had a lower risk of experiencing migraines.
Nonalcoholic fatty liver disease. In a study published in the European Journal of Nutrition, scientists from Columbia University examined 25 years of health data from 2,685 people and found that people in the top quintile of magnesium intakes were 55% less likely to develop the disease than people in the lowest intake quintile.
Stress. In a study published in the journal Stress and Health, people who had low magnesium levels and were under severe stress but were otherwise healthy took 300 mg of magnesium a day for eight weeks. Anxiety and depression scores significantly improved among the participants. “Magnesium supplementation … could provide a meaningful clinical benefit in daily life for individuals with stress and low magnesemia,” concluded the researchers.
Suboptimal Intake Is Common
Magnesium deficiency is uncommon, occurring in less than 2% of the population, says Dr. Rosanoff, but suboptimal intake is very common. According to the National Health and Nutrition Examination Survey, 79% of American adults do not meet their recommended daily allowance for magnesium: 400 to 420 for men and 310 to 320 for women—and these values, published in 1997, are low compared to the body’s need for magnesium.
“I consider the low intake of magnesium to be the single most important nutritional deficit in the United
States,” says Jacob Teitelbaum, MD, an internist in Kona, Hawaii. That’s because a low intake could be
playing a major role in the current epidemics of heart disease, stroke, and Type 2 diabetes, he notes.
Recommending a Supplement
Magnesium supplements are inexpensive and safe, says Dr. Rosanoff. For a person taking a magnesium supplement to prevent illness, Dr. Rosanoff recommends 350 mg daily. If your patient has a clinical issue that magnesium might help, such as high blood pressure or blood sugar levels, Dr. Rosanoff thinks 600 mg daily in a single dose before bedtime is agood recommendation.
If that amount produces loose stools—a possible side effect of magnesium supplementation—the patient should divide the amount into two 300 mg doses or three 200 mg doses. Or they should cut back on the single dose by 100 mg every few days, until their bowel movements normalize, Dr. Rosanoff notes.
Dr. Block routinely recommends 500 mg daily to her patients—increasing it gradually until the patient reaches bowel tolerance and then cutting back slightly until the bowel movements are again well-formed.
And don’t forget to remind patients to eat magnesium-rich foods, says Dr. Teitelbaum, who recommends leafy greens and nuts, especially almonds, as the best dietary sources of the mineral. Other foods rich in magnesium include dark chocolate, avocados, beans, whole grains, and bananas.
More information:
https://convenientcareclinician.com
Other resources:

by admin | Jul 26, 2021 | Magnesium Education
Vigorous activity can influence nutritional magnesium status, and magnesium status can influence physical performance as well as dictate whether vigorous physical activity is healthy or dangerous. This is true whether the runner is fit or unfit, trained or untrained.
Nutritional magnesium is deeply involved in ATP (energy) production, oxygen uptake, central
nervous function, electrolyte balance, glucose metabolism and muscle contraction, including the
all important muscles—the heart plus all its blood vessels.
During both a race and training, vigorous exercise ups the body’s requirement for nutritional
magnesium—not only because of the higher metabolism and muscle contraction where
magnesium plays crucial roles, but also because of increased magnesium loss in sweat and urine.
It has been estimated that athletes’ general requirement for nutritional magnesium is easily 10 –
20% higher than the general population. At the same time, nutritional magnesium can be low in
modern, processed food diets. Without a reliable, widely available marker for clinical
magnesium status (widely used serum magnesium reference ranges do not adequately reflect
body magnesium status), the combination of increased magnesium need for racing/training plus
marginal magnesium intake can make the seemingly healthy choice of running just the opposite
by depleting an already low body magnesium.
When magnesium status is healthy and adequate, blood magnesium shows large swings during
exercise, more than 10 times larger than when exercising in a marginal or deficient magnesium
state. This wide range of blood magnesium inflow and outflow enables the healthy body to fully
function during the high magnesium need of vigorous exercise. Healthy magnesium stores allow
for the large excretions of magnesium in urine and sweat that occur when the body is performing
at peak capacity–without danger of going into a depleted magnesium state. These magnesium
changes in blood and urine normalize within 24 hours after vigorous exercise in runners adequate
in magnesium, unless a deficit has been induced by the exercise bout. In runners with marginal
or deficit magnesium status, the blood levels do not show such wide swings of magnesium
during performance, and urine losses are smaller. It is as if the body is conserving its precious
store of magnesium by limiting the body’s ability to perform at its peak. Thus, it has been shown
that supplemental magnesium given to deficient and marginally deficient runners allows
measurably increased performance during athletic events, while those who are magnesium
adequate are already performing at peak ability which magnesium supplements do not enhance.
Reference: Nielsen FH, Lukaski HC. Update on the relationship between magnesium and exercise. Magnes Res 2006;19(3):180-9.http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=17172008
Source: CMER Center for Magnesium Education and Research
Contact: A. Rosanoff, Ph.D., Director of Research and Information Outreach
https://magnesiumeducation.com/